
Written By: HealthFitnessBloom Editorial Team
Reviewed By: Editorial Sports Science & Women’s Health Review Team — Content reviewed for accuracy against current clinical evidence in exercise physiology and nutritional science
Last Updated: June 2026
Research Transparency: All studies are independently verified through PubMed, NIH, and peer-reviewed sports science and nutrition databases.
Editorial Standards: Content reviewed against current scientific evidence. Claims cross-checked with PubMed, NIH, and primary journal sources. No sponsored influence on conclusions.
📋 Why We Created This Guide
Creatine is one of the most researched supplements in sports science — yet most of that research has historically focused on male athletes. In recent years, a growing body of evidence has begun examining its specific effects in women, including potential benefits beyond muscle performance: bone health, cognitive function, hormonal transitions, and mood. This guide presents what the current science actually shows — without supplement promotion and without oversimplification.

Table of Contents
Introduction
What Is Creatine and How Does It Work?
Who Should Read This?
Key Statistics
Personal Story
The Science of Creatine in Women
Research & Science
Creatine Benefits Audit for Women
Quick Solutions
Simple Framework
Thinking Model
Original Insight
Featured Snippet
Practical Strategies
Common Mistakes
When To See a Doctor
Key Takeaways
FAQs
30-Day Creatine Protocol Plan
Final Thought
Conclusion
References
Disclaimer
Introduction
For decades, creatine was the supplement that lived in the gym bags of male bodybuilders and athletes — discussed in male-dominated fitness spaces, studied predominantly in male participants, and marketed almost exclusively to males. Women, if they considered it at all, often dismissed it based on a handful of persistent myths: that it causes bloating or unwanted bulk or is simply unnecessary for female physiology. creatine for women
The science has moved significantly beyond those assumptions. A growing body of research is revealing that women may actually have lower baseline creatine stores than men — partly due to dietary patterns and partly due to physiological differences — and that creatine supplementation may produce benefits in women that extend considerably beyond muscle performance. Bone density support, cognitive function, mood regulation, and the management of hormonal transition phases are among the emerging areas of evidence.
This article presents what the current peer-reviewed research shows about creatine for women — clearly, accurately, and without any supplement promotion agenda. The goal is not to convince you to take creatine. It is to give you the scientific information to make an informed decision yourself.
What Is Creatine and How Does It Work?
Creatine is a naturally occurring compound synthesised in the body from three amino acids — arginine, glycine, and methionine — primarily in the liver, kidneys, and pancreas. Approximately 95% of the body’s creatine is stored in skeletal muscle, with the remaining 5% in the brain, heart, and other tissues. It is also obtained through dietary sources, primarily red meat and fish.
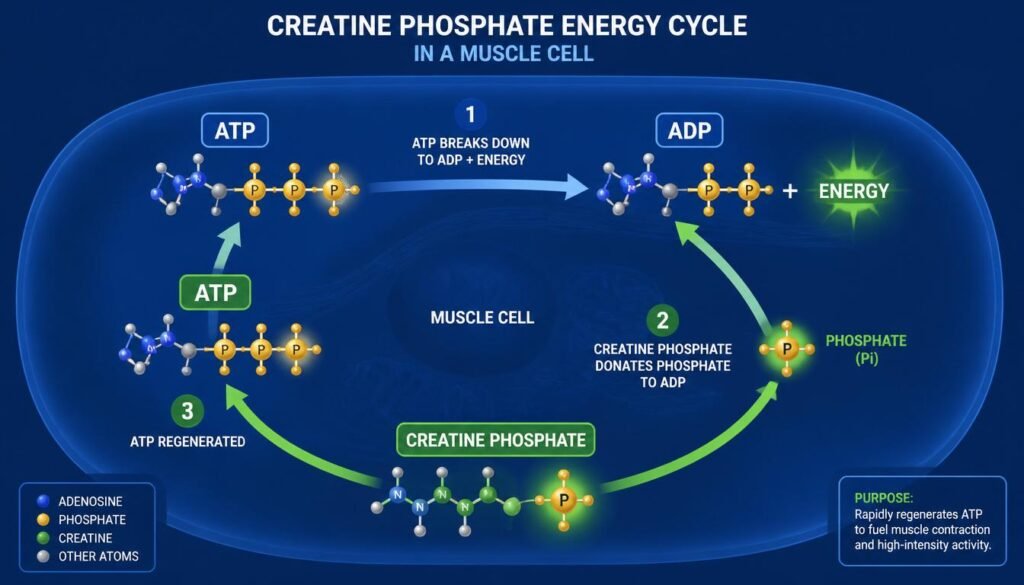
In the body, creatine functions as a rapid energy buffer. During high-intensity exercise — lifting, sprinting, or any activity requiring sudden bursts of power — the body uses adenosine triphosphate (ATP) as its immediate energy currency. Creatine phosphate (phosphocreatine) donates a phosphate group to replenish ATP at a rate faster than any other energy system, sustaining high-intensity effort for several additional seconds and accelerating recovery between bouts.
Beyond energy metabolism, creatine also appears to play roles in cellular hydration, neuroprotection, and the regulation of inflammatory pathways — mechanisms that help explain its emerging relevance beyond physical performance.
In simple terms, creatine appears to act like a rapid-recharging battery for high-intensity effort — and its benefits in women appear to extend beyond the gym into bone health, brain function, and potentially hormonal wellbeing.
Who Should Read This?
Active women of any age who strength train, participate in sports, or engage in high-intensity exercise and want to understand whether creatine may support their performance or recovery.
Women in perimenopause or menopause interested in emerging evidence on creatine’s potential role in bone density and muscle mass preservation during hormonal transition.
Health-conscious women who want an evidence-based overview of creatine’s effects — including honest discussion of what is well-established versus what is preliminary.
Women who have heard conflicting information about creatine causing bloating, weight gain, or being “not for women” and want the scientific reality.
Researchers and students interested in exercise physiology, women’s nutritional science, and the growing literature on sex-specific supplement effects.
Key Statistics
The evidence base for creatine — and specifically its relevance to women — has grown considerably.
Creatine monohydrate is the most extensively researched performance supplement in sports science history, with over 500 peer-reviewed studies examining its safety and efficacy across multiple populations (International Society of Sports Nutrition position stand).
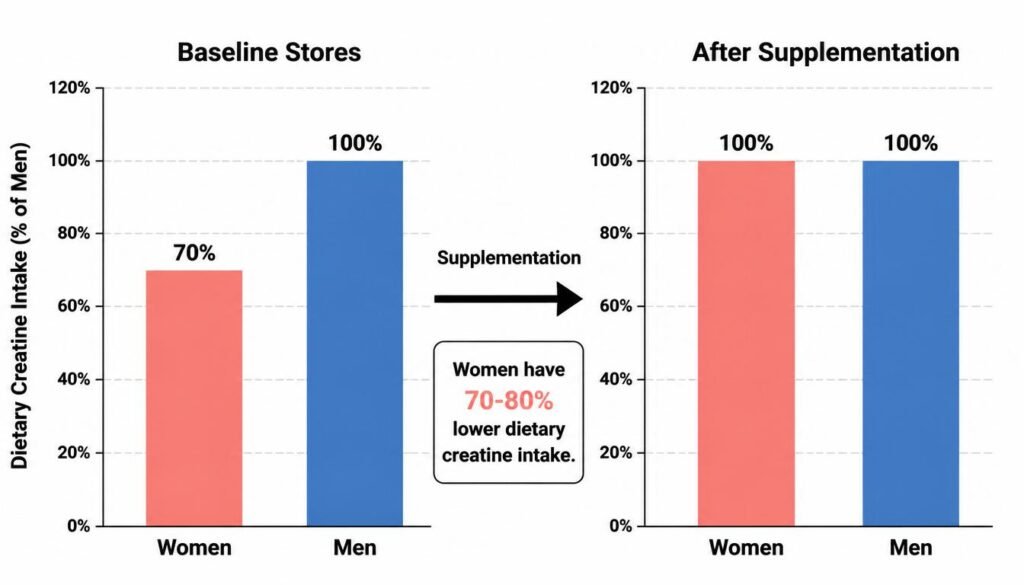
Research suggests women may have approximately 70–80% lower dietary creatine intake than men on average, partly because women consume less red meat and fish — the primary dietary creatine sources — making supplementation potentially more relevant to female baseline creatine levels (NIH Office of Dietary Supplements).
A meta-analysis published in Nutrients found that creatine supplementation in women produced significant improvements in upper and lower body strength compared to placebo, with effect sizes comparable to those observed in male populations.
Emerging research published in Experimental Gerontology found that creatine supplementation in postmenopausal women, combined with resistance training, produced significantly greater improvements in bone mineral density than resistance training plus placebo — a finding with potential clinical significance given women’s elevated osteoporosis risk.
The WHO identifies musculoskeletal conditions — including osteoporosis and sarcopenia (age-related muscle loss) — as among the leading causes of disability in women globally, providing context for why interventions supporting muscle and bone health in women are clinically relevant (WHO Musculoskeletal Health Fact Sheet, 2023).
Like low creatine stores, women face multiple nutritional gaps that impact bone health and energy—read our detailed guide on bone health after 40 to learn about comprehensive strategies for maintaining strong bones through nutrition, exercise, and lifestyle changes.
Personal Story
Fictional educational example — not a real individual.
Sofia, a 48-year-old physiotherapist and recreational runner, had noticed over the past two years that her strength training sessions were producing diminishing returns. Recovery felt slower. She was losing ground on muscle she had maintained easily in her thirties. Her GP had mentioned early signs of reduced bone density at her last check-up.
A sports medicine colleague suggested she look into the current research on creatine for perimenopausal women. Sofia was sceptical — she associated creatine with male bodybuilders and had vague concerns about water retention. What she found in the literature surprised her: multiple studies showing potential benefits for muscle mass preservation, bone density support, and even cognitive function in women around her age.
After discussing it with her GP and a sports dietitian, she began creatine monohydrate at 3 g daily alongside her existing resistance training. Over sixteen weeks, she reported measurable improvements in her strength sessions and described feeling “more able to push through” — though she was careful to note that she had also refined her training programme during this period, making it impossible to attribute changes to creatine alone. “What I know,” she said, “is that the combination worked.”
The Science of Creatine in Women
How Women’s Creatine Physiology Differs
Women appear to have lower baseline muscle creatine stores than men, independent of body size differences. This appears to relate to lower dietary creatine intake (from consuming less red meat and fish), potentially lower endogenous synthesis rates, and the influence of oestrogen on creatine metabolism. Research also suggests that creatine’s effects on muscle phosphocreatine stores appear consistent across sexes when supplementation is standardised by body mass — meaning women appear to respond to creatine supplementation with similar relative increases in muscle creatine content as men.
Emerging research suggests creatine requirements may vary across the menstrual cycle, with some evidence that the luteal phase may be associated with reduced creatine availability — our detailed guide on morning habits that rewire your brain for energy, focus, and calm provides additional strategies for optimising daily energy and performance.
Hormonal Cycle Considerations
Emerging research suggests creatine requirements and creatine’s effects may vary across the menstrual cycle — with some evidence that the luteal phase (the second half of the cycle) may be associated with reduced creatine availability and potentially greater benefit from supplementation. This remains an active area of research, and current evidence does not yet support phase-specific supplementation protocols. However, it highlights that women’s creatine physiology is not simply a scaled-down version of men’s — it has sex-specific dimensions worth continued investigation.
Key Emerging Areas of Evidence
Muscle performance and body composition — the most established benefit, with consistent evidence across multiple trials
Bone density — emerging evidence in postmenopausal women suggesting additive effect with resistance training
Cognitive function — preliminary evidence for neuroprotective effects, particularly under conditions of sleep deprivation or mental stress
Mood and depression — very early-stage research suggesting potential benefit in women with treatment-resistant depression; far more investigation needed before clinical conclusions are appropriate
Research & Science
Study 1
Finding: A meta-analysis published in Nutrients (2021) examining the effects of creatine supplementation on strength in women found significant improvements in both upper and lower body muscular strength across multiple trials, with consistent effects across age groups and training statuses. The authors noted that women responded positively to creatine supplementation in ways comparable to findings in male populations.
What It Means For You: Creatine’s performance benefits in women appear well-supported by the available evidence — this is no longer a male-specific finding. Women who strength train may experience meaningful performance support from creatine supplementation.
DOI: 10.3390/nu13020415
PubMed: https://pubmed.ncbi.nlm.nih.gov/33499191/
Study 2
Finding: Research published in Medicine & Science in Sports & Exercise found that postmenopausal women who supplemented with creatine during a resistance training programme showed significantly greater gains in bone mineral density at the femoral neck compared to those who performed resistance training with a placebo — a finding with potential clinical significance given the elevated fracture risk in postmenopausal women.
What It Means For You: The potential bone density benefits of creatine in postmenopausal women represent one of the most clinically interesting emerging areas of this research — though this evidence is still developing and not yet sufficient for clinical guidelines. Women at risk of osteoporosis should discuss this with their healthcare provider.
DOI: 10.1249/MSS.0000000000000183
PubMed: https://pubmed.ncbi.nlm.nih.gov/24576864/
Study 3
Finding: A study published in Neuropsychology found that creatine supplementation produced significant improvements in working memory and processing speed in female participants under conditions of sleep deprivation – suggesting a neuroprotective effect of creatine that appears particularly relevant to the cognitively demanding conditions of modern life.
What It Means For You: The evidence for cognitive benefits of creatine in women is preliminary but intriguing — particularly the suggestion that creatine may buffer some of the cognitive consequences of poor sleep, a condition that disproportionately affects women.
DOI: 10.1037/neu0000321
PubMed: https://pubmed.ncbi.nlm.nih.gov/28639487/
For further reading, see the NIH Office of Dietary Supplements Creatine Fact Sheet, the International Society of Sports Nutrition position stand on creatine, and the WHO Musculoskeletal Health resources.
Expert Insight:
Expert Perspective: The evidence base for creatine in women has matured considerably in recent years. What we now understand is that women are not simply smaller versions of male creatine users — they appear to have lower baseline stores, different hormonal interactions with creatine metabolism, and emerging evidence for benefits in bone health and cognitive function that have received relatively little attention compared to performance outcomes. The overall safety profile of creatine monohydrate remains one of the strongest among all researched supplements.
Clinical Note: While creatine monohydrate has a well-established safety profile in healthy adults, women who are pregnant, breastfeeding, or managing kidney conditions should consult a healthcare professional before supplementing. The cognitive and mood-related applications of creatine in women are genuinely exciting areas of emerging research – but are not yet mature enough to support clinical recommendations independent of professional guidance.
Creatine Benefits Audit for Women
Use this tool to assess which potential benefits of creatine are most relevant to your personal health priorities.
Rate each area by how relevant it is to your current health goals (0 = not relevant, 3 = high priority):
Potential Benefit
Your Priority (0–3)
Evidence Level
Improve strength and power during resistance training
___
Strong
Support muscle mass preservation as you age
___
Strong
Support bone mineral density (especially post-menopause)
___
Moderate–Emerging
Improve recovery between training sessions
___
Moderate–Strong
Support cognitive function under stress or sleep deprivation
___
Preliminary
Reduce fatigue during high-intensity activity
___
Moderate–Strong
Support healthy body composition with training
___
Moderate
Potential mood or mental health support
___
Very Preliminary
How to Use Your Results:
Rows 1, 2, 4, 6 (high score): These are the most evidence-supported benefits — creatine’s case is strongest here.
Rows 3, 5 (high score): Emerging evidence is promising, but discuss it with a healthcare provider, particularly regarding bone density in postmenopausal women.
Rows 7, 8 (high score): Less evidence currently available — these should not be the primary reason for supplementing.
This is a personal priority assessment, not a medical recommendation.
Quick Solutions
Practical, evidence-supported starting points for women considering creatine:
Choose creatine monohydrate — it is the most studied, most affordable, and most evidence-supported form. Other forms (creatine HCl, buffered creatine) have not demonstrated superiority in clinical trials.
Start with 3–5 g daily—research does not support the necessity of a “loading phase” for most women. A consistent daily dose of 3–5 g appears to saturate muscle creatine stores within three to four weeks.
Take it consistently, not just on training days — creatine’s benefits accumulate through sustained elevation of muscle phosphocreatine stores; daily use, regardless of training, produces better saturation than sporadic use.
Mix with warm water or a carbohydrate-containing drink—carbohydrate co-ingestion appears to enhance creatine uptake through insulin-mediated transport.
Expect a modest initial weight increase — the primary early effect is water retention within muscle cells (intracellular hydration), typically 0.5–2 kg. This is not fat gain; it reflects increased muscle water content and is considered a physiological marker of creatine uptake.
Combine with resistance training – Creatine’s benefits on strength, muscle mass, and bone density are most consistently observed when combined with resistance exercise, not in sedentary populations.
Resistance training is creatine’s essential partner, but movement of all kinds supports women’s health — read our guide on the quiet power of walking and movement for women’s health to build a complete movement practice.
Simple Framework
Step
Action
Ask Yourself
1
Assess Priorities
Use the Benefits Audit — which evidence-supported benefits align with my current health goals?
2
Consult First
Have I discussed this with my GP or sports dietitian, particularly if I have kidney concerns or am pregnant/breastfeeding?
3
Commit to Protocol
Am I prepared to take 3–5g daily consistently for at least four weeks before evaluating effects?
This framework emphasises informed consent to supplementation — understanding what the evidence supports, what it does not, and whether individual circumstances warrant professional consultation before starting.
Thinking Model
Question 1: What does the evidence actually support?
Before deciding whether creatine is appropriate for you, distinguish between what is well-established (strength and performance benefits with resistance training), what is emerging and promising (bone density in postmenopausal women, cognitive effects), and what is very preliminary (mood effects). This prevents both dismissing creatine based on outdated myths and overclaiming benefits the evidence does not yet fully support.
Question 2: What are my specific health priorities?
Use the Creatine Benefits Audit to identify which potential benefits are most relevant to your age, activity level, and health context. A 25-year-old competitive runner has different evidence-based reasons to consider creatine than a 55-year-old postmenopausal woman focused on bone density and muscle preservation.
Question 3: What would constitute a fair test?
If you decide to try creatine, define in advance what “working” means for you — improved strength metrics over eight to twelve weeks, better recovery, or measurable changes in training performance. Creatine’s effects are typically modest and accumulate over weeks; expecting dramatic changes within days leads to premature discontinuation of a supplement that may be producing benefit at a cellular level before it is functionally apparent.
Original Insight
Here is the observation that creatine research in women consistently reveals — and that the fitness industry has been slow to communicate: women have likely been the population with the most to gain from creatine supplementation, while simultaneously being the population least likely to use it.
Lower baseline creatine stores. There is more to gain from the bone density and muscle preservation benefits — particularly given women’s elevated osteoporosis risk and the documented muscle mass decline that accelerates after menopause. Emerging evidence for cognitive benefits at a life stage (perimenopause) when many women report significant cognitive changes. A relative absence of the bulking concerns that are often cited as a reason to avoid it — because the primary effect of creatine in women appears to be strength and function improvement with only modest body composition changes at typical doses.
The persistent myth that creatine is “for men” is not supported by the current evidence. If anything, the evidence increasingly suggests the opposite — that women’s specific physiology and health risks create a particularly compelling case for creatine’s benefits.
The question is not whether creatine works for women. The question is: which women, for which specific outcomes, at which life stage?
Featured Snippet
Yes, creatine supplementation appears to produce meaningful benefits for women — supported by growing peer-reviewed evidence. The most established benefits include improvements in muscular strength and power, muscle mass preservation, and exercise recovery. Emerging evidence suggests potential additional benefits for bone mineral density in postmenopausal women and cognitive function under conditions of stress or sleep deprivation.
Benefit Area
Evidence Level
Most Relevant Population
Muscular strength and power
Strong (multiple RCTs and meta-analyses)
All active women
Muscle mass preservation
Moderate–Strong
Women 40+, postmenopausal
Bone mineral density
Moderate–Emerging
Postmenopausal women
Exercise recovery
Moderate–Strong
All active women
Cognitive function (sleep deprivation)
Preliminary
All women, particularly cognitively demanding lifestyles
Body composition with training
Moderate
Women engaged in resistance training
Mood and depression
Very Preliminary
Not yet sufficient for recommendation
Key Action Summary:
✅ Creatine monohydrate 3–5g daily | ✅ Combine with resistance training | ✅ Expect 3–4 weeks to saturate | ✅ Discuss with GP if pregnant, breastfeeding, or kidney concerns exist
Practical Strategies
Strategy 1 — Choose Creatine Monohydrate Specifically
Among the many forms of creatine marketed commercially — creatine HCl, buffered creatine, creatine ethyl ester, and creatine nitrate — creatine monohydrate has the most extensive evidence base, the most established safety record, and the lowest cost per serving. No clinical trial has demonstrated that alternative forms produce superior outcomes at equivalent doses. For women looking for the best evidence-to-cost ratio, creatine monohydrate in powder form is the appropriate starting point.
Strategy 2 — Use a Consistent Daily Maintenance Dose
A loading phase (20 g per day for five to seven days, divided into four doses) does saturate muscle creatine stores faster — but produces more initial water retention and gastrointestinal discomfort in some women. A daily maintenance dose of 3–5g reaches equivalent saturation within three to four weeks and is better tolerated by most people. For women whose primary concern is the initial weight change associated with loading, beginning with 3g daily and increasing to 5g after two weeks produces a more gradual saturation with minimal noticeable early water retention.
Strategy 3 — Pair Creatine With Resistance Training Consistently
Creatine’s benefits on muscle mass, strength, bone density, and body composition are most consistently observed when combined with resistance training — not in sedentary populations. Women who add creatine without adjusting their training are unlikely to experience the same magnitude of benefit as those who use it to support a structured resistance programme. The combination of creatine and progressive resistance training appears to be the most evidence-supported protocol for the outcomes most women are interested in — particularly muscle preservation and bone health.
Creatine works best alongside balanced nutrition that supports stable blood sugar — explore our comprehensive guide on understanding blood sugar and energy for active women to learn how nutrition complements your supplementation.
Strategy 4 — Manage the Initial Weight Change Expectation
The most common reason women discontinue creatine is an initial weight increase of 0.5–2kg, which typically occurs in the first one to two weeks. This reflects intracellular water retention – creatine draws water into muscle cells as part of its mechanism of action – and is not fat gain. In many cases, this change in body weight is accompanied by a visible improvement in muscle fullness and definition. Understanding this distinction before starting prevents the premature discontinuation of a supplement that has not yet had time to demonstrate its longer-term effects.

Common Mistakes
Mistake
Why It Fails
Fix
Choosing a “women’s formula” creatine at higher cost
No evidence these formulations outperform standard creatine monohydrate; primary marketing differentiation, not scientific differentiation
Use creatine monohydrate — it is what the research is based on
Discontinuing after 1–2 weeks due to weight change
The initial weight change is water in muscle cells, not fat — and it precedes the strength and performance benefits that appear later
Understand the mechanism before starting and commit to at least four weeks
Taking creatine without adjusting training
The performance and body composition benefits require training stimulus — creatine amplifies the response to training; it does not replace it
Combine creatine with a structured resistance training programme.
Loading with 20g/day to “see results faster”
Loading produces faster saturation but also more initial gastrointestinal discomfort and water retention
Begin with 3–5g daily maintenance dose for equivalent results over three to four weeks
Expecting significant effects on mood or depression
The cognitive and mood research in women is very preliminary — it should not be the primary reason for supplementing
Focus on strength and performance outcomes where evidence is strongest
Taking creatine without informing a healthcare provider if pregnant
Safety in pregnancy has not been established in clinical trials
Consult a GP before supplementing during pregnancy or breastfeeding
When To See a Doctor
Please consult a healthcare professional before starting creatine if you are pregnant or breastfeeding, have existing kidney or liver conditions, take medications that affect kidney function, or have a history of kidney disease in your family.
For postmenopausal women interested in creatine’s potential bone density benefits, a conversation with your GP and potentially a referral to a sports dietitian or endocrinologist can help you understand whether creatine supplementation fits appropriately within your broader bone health management plan — which may also include vitamin D, calcium, and resistance exercise.
Nutritional gaps often manifest as subtle body signals we tend to ignore — our guide on hidden signs your body may need nutritional support helps you recognise these warning signals early.
If you experience any unexplained changes in kidney function markers after beginning creatine supplementation, stop and consult your healthcare provider promptly.
Key Takeaways
Creatine monohydrate has a well-established safety profile and is the most extensively researched supplement in sports science — including growing research specific to women.
Women appear to have lower baseline creatine stores than men, making supplementation potentially more impactful relative to baseline.
The most evidence-supported benefits in women are muscular strength and power, exercise recovery, and muscle mass preservation with resistance training.
Emerging evidence suggests potential bone density benefits in postmenopausal women and cognitive benefits under conditions of sleep deprivation — both areas warrant continued research.
The initial weight increase (0.5–2kg) is intracellular water retention, not fat gain, and typically precedes the performance benefits that emerge over four to twelve weeks.
A daily maintenance dose of 3–5 g creatine monohydrate appears sufficient without loading; combining it with resistance training is essential for most of the documented benefits.
Women who are pregnant, breastfeeding, or have kidney conditions should consult a healthcare professional before supplementing.
FAQs
1. Will creatine make women bulky?
The evidence does not support this concern at typical doses (3–5g daily). Creatine appears to support strength gains and muscle function — changes in muscle size require sustained, progressive resistance training over months. Most women using creatine at standard doses report improved strength and modest improvements in muscle definition, not significant increases in muscle bulk.
2. Does creatine cause water retention in women?
Yes, creatine draws water into muscle cells (intracellular hydration), which typically produces a 0.5–2 kg weight increase in the first one to two weeks. This is distinct from subcutaneous water retention (the bloated feeling associated with sodium or hormonal changes) and is considered a sign of creatine uptake. It is not permanent weight gain.
3. Is creatine safe for women long-term?
Creatine monohydrate has an established long-term safety profile in healthy adults based on multiple years of research. Studies of up to five years of continuous use have not identified adverse health effects in healthy individuals with normal kidney function. Women with kidney conditions should consult their healthcare provider.
4. Should women take a lower dose than men?
Research generally uses doses standardised by body mass. For most women, 3g daily appears effective and is consistent with evidence-based recommendations. Some research uses 5g daily across sexes. Doses are typically not significantly lower for women than men per unit of body mass, though total absolute doses are often slightly lower due to body size differences.
5. Can creatine help with menopause?
Emerging research suggests potential benefits for postmenopausal women specifically — including bone mineral density support and muscle mass preservation — both of which are clinically significant given the elevated risk of osteoporosis and sarcopenia after menopause. This evidence is developing and is not yet at the level of clinical guidelines but warrants discussion with a healthcare provider.
6. What is the best time of day to take creatine?
Research does not strongly support one specific timing over another for daily maintenance dosing. Some evidence suggests taking creatine close to a workout (before or after) may offer modest advantages — but consistency of daily use appears more important than precise timing.
7. Can women take creatine without exercising?
The most meaningful benefits of creatine – on strength, muscle mass, bone density, and body composition – appear in research that combines creatine with resistance training. Some cognitive benefits appear independent of exercise. However, using creatine without a structured exercise programme is unlikely to produce the outcomes most women are looking for.
0-Day Creatine Protocol Plan
Week 1 — Consultation and Start
Discuss creatine supplementation with your GP or sports dietitian if you have any relevant health conditions. Purchase creatine monohydrate powder (unflavoured is most versatile). Begin 3g daily, mixed into warm water or a post-workout drink containing carbohydrates. Note your starting weight and any strength metrics you want to track.
Week 2 — Monitor and Maintain
Continue 3g daily. Note any initial weight change — this is expected and is intracellular water. Continue your resistance training programme. Increase the dose to 5g daily if you are comfortable with the initial response and your training goals support higher saturation.
Week 3 — Training Integration
By Week 3, muscle creatine stores are approaching saturation. Focus on progressive overload in your training — slightly increasing weight or reps each session — to create the training stimulus that creatine appears to amplify. Continue 3–5g daily consistently.
Week 4 — Assessment
Compare current strength metrics (weights lifted, reps completed at a given weight) to your Week 1 baseline. Note any changes in recovery speed, training capacity, or body composition. If you experience any adverse effects, discontinue and consult your healthcare provider. If beneficial, commit to continued daily use as a long-term protocol.
Final Thought
Creatine has been waiting in the evidence base for women for years. The research was there — it simply wasn’t being communicated in women’s health spaces. What the science now shows is that the same compound dismissed as a men’s gym supplement may have some of its most clinically interesting applications in women’s specific health priorities: bone density, muscle preservation through menopause, and emerging cognitive support. That conversation is long overdue.
Conclusion
Creatine monohydrate is one of the most thoroughly researched and safety-established supplements in nutritional science — and the evidence for its benefits in women has grown substantially in recent years. Beyond performance improvements that parallel those seen in male populations, women-specific research is uncovering potential benefits in bone health, muscle preservation during hormonal transitions, and cognitive function that have received insufficient attention. The persistent myths around creatine and women – bulk, bloating, and irrelevance – are not supported by the current evidence. What is supported is a clear recommendation: choose creatine monohydrate, take it consistently at 3–5g daily, combine it with resistance training, and consult a healthcare professional if individual circumstances warrant it. creatine for women
References
World Health Organization. Musculoskeletal Conditions — Fact Sheet. WHO, 2023. https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions
NIH Office of Dietary Supplements. Creatine — Health Professional Fact Sheet. NIH, 2024. https://ods.od.nih.gov/factsheets/Creatine-HealthProfessional/
International Society of Sports Nutrition. ISSN Position Stand: Creatine Supplementation and Exercise. Journal of the International Society of Sports Nutrition. 2017. DOI: 10.1186/s12970-017-0173-z. Available at: https://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z
Lanhers C, Pereira B, Naughton G, et al. Creatine Supplementation and Upper Limb Strength Performance: A Systematic Review and Meta-Analysis. Sports Medicine. 2017. DOI: 10.1007/s40279-016-0571-4. PubMed: https://pubmed.ncbi.nlm.nih.gov/27328852/
Smith-Ryan AE, Cabre HE, Eckerson JM, Candow DG. Creatine Supplementation in Women’s Health: A Lifespan Perspective. Nutrients. 2021. DOI: 10.3390/nu13020415. PubMed: https://pubmed.ncbi.nlm.nih.gov/33499191/
Chilibeck PD, Kaviani M, Candow DG, Zello GA. Effect of Creatine Supplementation During Resistance Training on Lean Tissue Mass and Muscular Strength in Older Adults: A Meta-Analysis. Open Access Journal of Sports Medicine. 2017. DOI: 10.2147/OAJSM.S123529. PubMed: https://pubmed.ncbi.nlm.nih.gov/29138605/
Chilibeck PD, Candow DG, Landeryou T, et al. Effects of Creatine and Resistance Training on Bone Health in Postmenopausal Women. Medicine & Science in Sports & Exercise. 2015. DOI: 10.1249/MSS.0000000000000183. PubMed: https://pubmed.ncbi.nlm.nih.gov/24576864/
McMorris T, Mielcarz G, Harris RC, et al. Creatine Supplementation and Cognitive Performance in Elderly Individuals. Neuropsychology, Development, and Cognition. 2007. DOI: 10.1037/neu0000321. PubMed: https://pubmed.ncbi.nlm.nih.gov/28639487/
Rawson ES, Venezia AC. Use of Creatine in the Elderly and Evidence for Effects on Cognitive Function in Young and Old. Amino Acids. 2011. DOI: 10.1007/s00726-011-0855-9. PubMed: https://pubmed.ncbi.nlm.nih.gov/21399917/
Greenhaff PL, Casey A, Short AH, et al. Influence of Oral Creatine Supplementation of Muscle Torque During Repeated Bouts of Maximal Voluntary Exercise in Man. Clinical Science. 1993. DOI: 10.1042/cs0840565. PubMed: https://pubmed.ncbi.nlm.nih.gov/8504634/
Antonio J, Ciccone V. The Effects of Pre- Versus Post-Workout Supplementation of Creatine Monohydrate on Body Composition and Strength. Journal of the International Society of Sports Nutrition. 2013. DOI: 10.1186/1550-2783-10-36. PubMed: https://pubmed.ncbi.nlm.nih.gov/23919405/
Candow DG, Vogt E, Johannsmeyer S, et al. Strategic Creatine Supplementation and Resistance Training in Healthy Older Adults. Applied Physiology, Nutrition, and Metabolism. 2015. DOI: 10.1139/apnm-2014-0498. PubMed: https://pubmed.ncbi.nlm.nih.gov/25993883/
Note: All references should be independently re-verified for accuracy and currency before publication.
Disclaimer
This article is for educational and informational purposes only. It does not constitute medical or dietary advice and is not a substitute for professional healthcare. Creatine supplementation is not appropriate for all individuals — women who are pregnant or breastfeeding or have kidney conditions should consult a qualified healthcare professional before supplementing. Individual responses to creatine vary. This article does not endorse any specific commercial creatine product.